The alert raised by the WHO (World Health Organization) (1) and BHVI (Brien Holden Vision Institute) of myopia epidemic (4) is not just a prospective estimate without consequences. In fact, a myopic person has an increased risk factor of developing cataracts, glaucoma, retinal detachment, myopic maculopathy. Furthermore, this risk increases proportionally with magnitude of myopia. For example, the probability of having a retinal detachment is 3 times greater for a -1/-3 diopter myopic (compared with an emmetrope), and 44 times greater for a -7 diopter myopic (2). Given this increased risk of developing eye diseases, even some governments are concerned about their health care spending and are planning measures in this regard.
Considering all the above, this epidemic has also ethical relevance for vision healthcare professionals, who cannot ignore myopia management options: prescribing a single vision lens to a child with progressive myopia is clinically obsolete (5).
ProCrea Tech has significantly improved previous freeform lens designs for myopic progression. In fact, MYOCONTROL’s defocus distribution results both rapid lens adaptation and reduction in myopia progression. Its design exploits peripheral myopic defocus principle, which stems from understanding of human emmetropization process. Thanks to MYOCONTROL, all laboratories will finally be able to fulfill this ever-growing demand of the ophthalmic market and have a role in slowing down the myopia epidemic.
Scientific Background
After years of scientific research, it is now clear that eyeball myopization process is a biological mechanism that occurs locally in the retina. In particular, cells in the retinal periphery trigger the stimulus to elongate bulb tissues (3). Although there are numerous factors correlated with bulb myopization (genetic factors, time spent outdoors (6), near work (7), accommodative lag (8) and binocular vision (9)) these cells respond primarily to peripheral retinal defocus (3). Measuring peripheral defocus in myopes yields a hypermetropic value (10), which is also confirmed by mathematical models (11). This defocus is certainly one of the main stimuli for bulb elongation (3) and this is why undercorrecting myopia or using classic spherical lens designs is not helpful, indeed it may even worsen bulb elongation (12).
Myocontrol Design
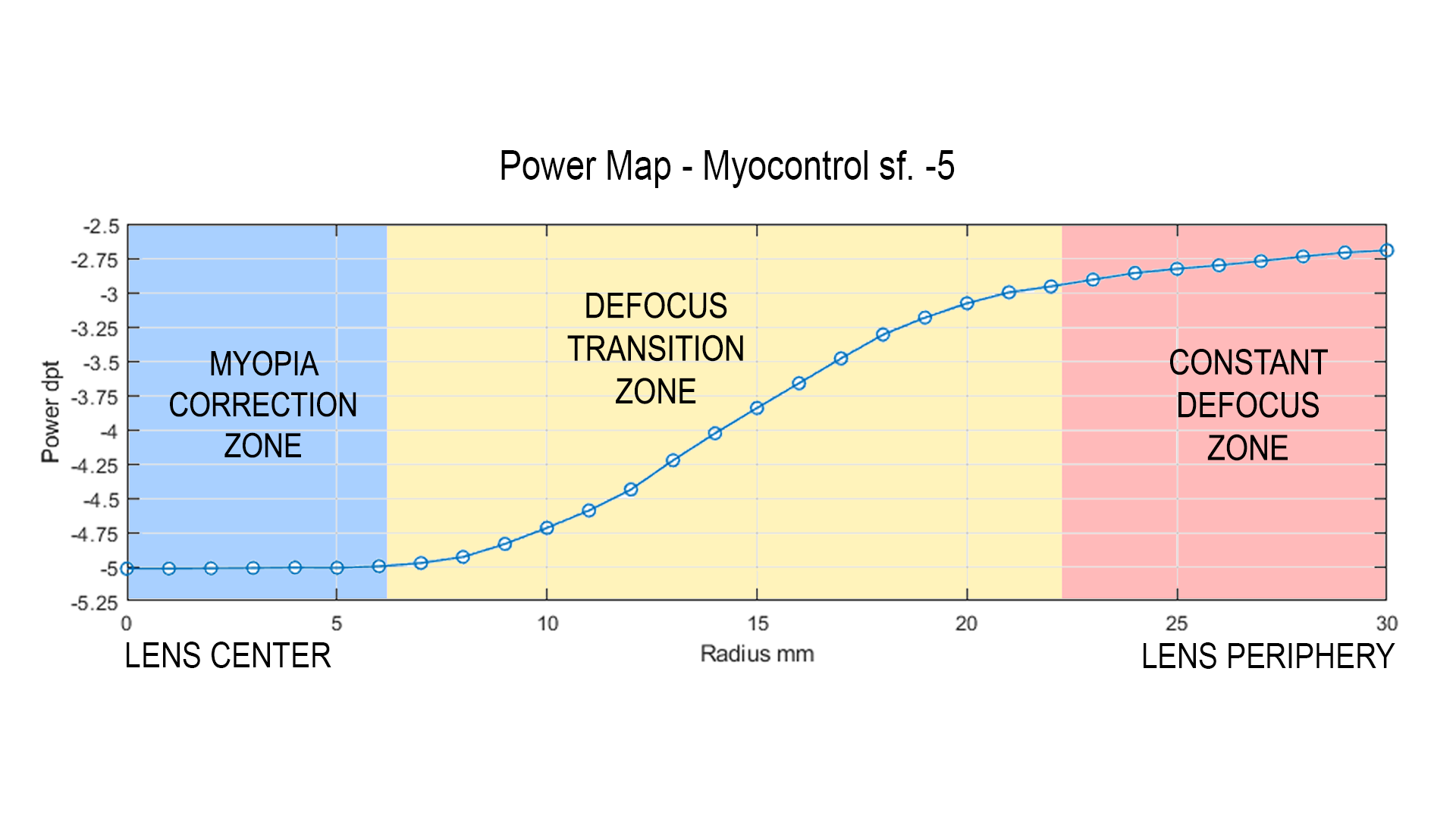
Based on this scientific background, ProCrea Tech has developed MYOCONTROL, which has a peripheral defocus up to +3 diopters, designed to control the stimulus of bulb elongation. Its design is accomplished through the well-known FreeForm optimization algorithms developed by ProCrea, and it can be schematized in three optical zones:
- The lens central zone is 12 mm wide and it has a negative optical power that compensates myopia and ensures sharp vision;
- From this point on, addition power increases and reaches from +2 to +3 diopters, depending on the degree of myopia. This zone is the defocus transition zone and and extends about 22 mm from the center of the lens;
- The last zone is a constant defocus zone. In fact, in this zone the addition power does not undergo rapid changes as in the previous zone, in order not to interfere excessively with the nervous coordination of wearer’s oculomotor system while ensuring sufficient defocus.
Efficacy And Other Solutions
There is widespread agreement in scientific literature on the effectiveness of contact lenses desined for myopia control, both soft and rigid ones (orthokeratology) (13). Almost all of them rely on the same principle of inducing myopic defocus on the retinal periphery in order to compensate for hypermetropic defocus that stimulates bulb elongation. Nowadays, as we have seen, it is possible to achieve a similar defocus values with FreeForm ophthalmic lenses, and eye care clinician will prescribe the most appropriate treatment on a case-by-case basis.A lens design similar to MYOCONTROL showed an effect in reducing myopia progression in a control group study (14), and because our design has higher and better distributed defocus values than the one tested, it is possible to expect increased effectiveness.
Bibliography
- World Health Organization. Report: The impact of myopia and high myopia. 2016.
- The complex interactions of retinal, optical and environmental factors in myopia aetiology. DI., Flitcroft. 31, s.l. : Progress in Retinal and Eye Research, 2012.
- IMI – Report on Experimental Models of Emmetropization. Troilo D, Smith EL III, Nickla DL, et al. 3, s.l. : IOVS, 2019, Vol. 60.
- Global Prevalence of Myopia and High Myopia and Temporal Trends from 2000 through 2050. A. Holden, Brien et al. 2016, Ophthalmology, pp. 1036-1042.
- World Council of Optometry. Resolution: The Standard of Care For Myopia Management by Optometrists. 2021.
- Time spent in outdoor activities in relation to myopia prevention and control: a meta‐analysis and systematic review. Xiong, Shuyu et al. 6, 2017, Vol. 95.
- Role of near work in myopia: findings in a sample of Australian school children. Jp JM, Saw SM, Rose KA, Morgan IG, Kifley A. Wang JJ, Mitchell P. 7, s.l. : IOVS, 2008, Vol. 49.
- Accommodative lag under habitual seeing conditions: Comparison between myopic and emmetropic. Nakatsuka C, Hasebe S, Nonaka F, Ohtsuki H. s.l. : Japanese Journal of Ophthalmology, 2005, Vol. 49.
- IMI – Accommodation and Binocular Vision in Myopia Development and Progression. Logan, Nicola S et al. 5, s.l. : Investigative ophthalmology & visual science, 2021, Vol. 62.
- Refractive Error, Axial Length, and Relative Peripheral Refractive Error before and after the Onset of Myopia . al., Donald O. Mutti et. 6, s.l. : IOVS, 2007, Vol. 48.
- Optical models for human myopic eyes. Atchison, David A. s.l. : Vision Research, 2006, Vol. 46.
- Interventions to slow progression of myopia in children. Walline JJ, Lindsley K, Vedula SS, Cotter SA, Mutti DO, Twelker JD. s.l. : Cochrane Database Syst Rev., 2011, Vol. 12.
- Efficacy Comparison of 16 Interventions for Myopia Control in Children: A Network Meta-analysis. Huang J, Wen D, Wang Q, McAlinden C, Flitcroft I, Chen H, Saw SM, Chen H, Bao F, Zhao Y, Hu L, Li X, Gao R, Lu W, Du Y, Jinag Z, Yu A, Lian H, Jiang Q, Yu Y, Qu J. 4, s.l. : Ophthalmology, 2016, Vol. 123.
- Spectacle Lenses Designed to Reduce Progression of Myopia: 12-Month Results. Sankaridurg P, Donovan L, Varnas S, Ho A, Chen X, Martinez A, Fisher S, Lin Z, Smith EL 3rd, Ge J, Holden B. 9, s.l. : Optometry and Vision Science, 2010, Vol. 87.